
SUMMARY: A staffing problem inside a hospital often has its origin one step upstream, in privileging. When a credential or a privilege update lands a day after the coverage decision is made, the cost looks like a supply or scheduling issue. The actual breakdown is in what was visible to the people making the call.
The framing that keeps breaking down in practice
For the first fifteen or so years of my career in healthcare SaaS, I watched health systems and staffing organizations build technology layer by layer, each tool solving one problem well and creating three new handoff points in the process. Credentialing platforms got better. Scheduling tools got better. They just didn't get better together.
Privileging got treated as a pre-game step. Something that happens before the real work starts. You clear it, you move on.
The pattern I keep coming back to is how often that framing breaks down in the field. Privileging doesn't sit cleanly upstream of staffing. It runs alongside it, and the gap between the two is where capacity quietly disappears.
I'm in a lot of operational conversations across health systems, group practices, and the agencies working alongside them. Those conversations almost always open on the same surface: a hard-to-fill shift, an external placement that came in over budget, a coverage gap that keeps reappearing on the same unit. When you trace it back, the trail usually leads through a credential that arrived late, an off-cycle privilege update nobody saw, or an eligibility change that didn't reach the scheduling view in time. By then, the decision had already been made.
The credential that lands a day late
The most common version of this is small enough to feel routine.
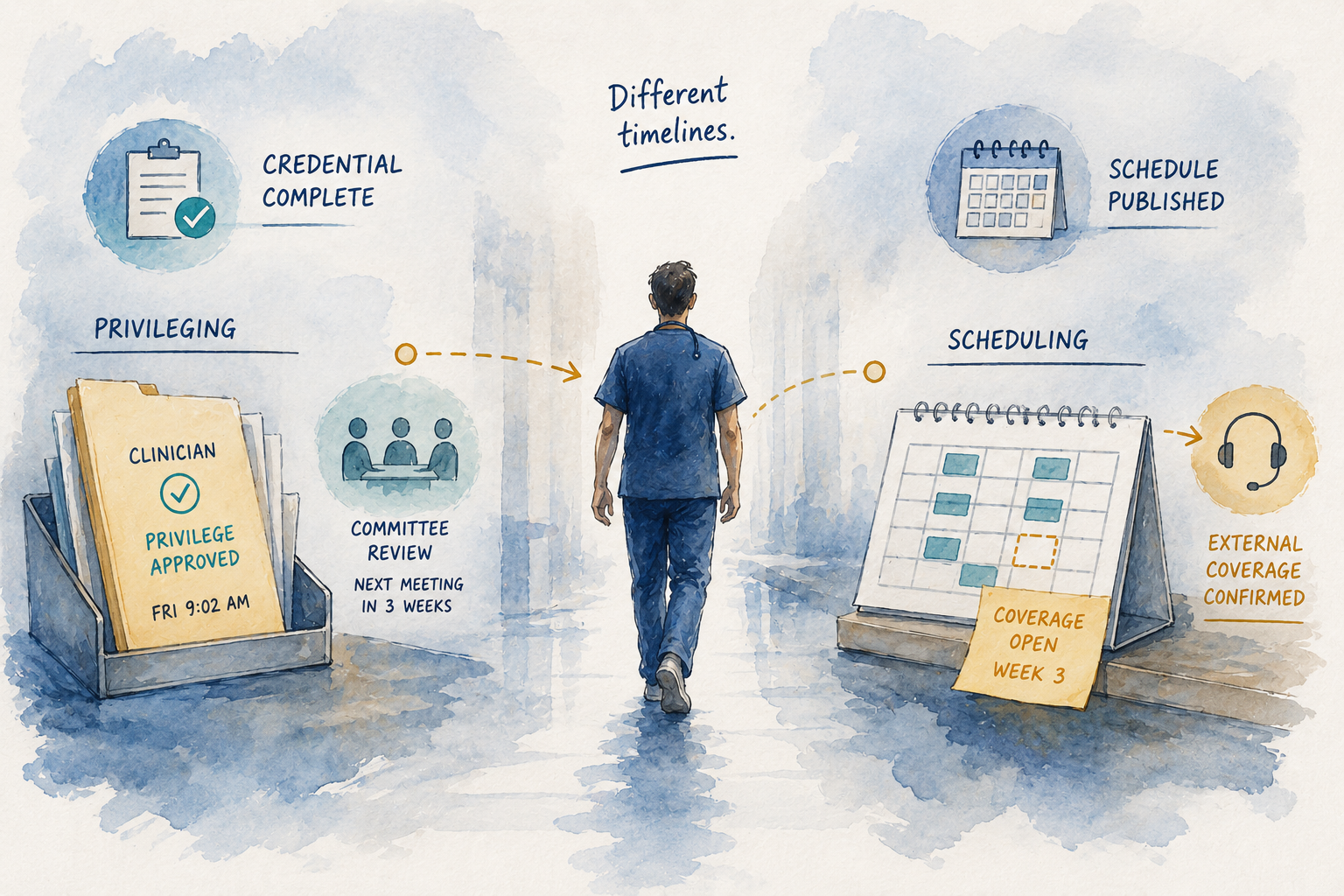
A clinician completes credentialing on a Tuesday. The privilege update is approved later that week. The information moves through the systems it's supposed to move through. By Friday morning, the eligibility status is current in the credentialing platform.
The scheduling team made a Thursday afternoon decision on the open shift that clinician could have filled.
No one did anything wrong. The clinician was ready. The credentialing team did their job. The scheduler made the call on the information she could see, because schedulers don't work from "almost ready." They work from what they can confirm. The decision just sat one day ahead of the data.
This is not a rare edge case. In most organizations I talk to, it is a recurring one. And the operational reality is that nobody gets paged about it. The scheduler fills the shift. The week moves on. The variance shows up later, in a report that reads as a staffing cost issue, not a privileging visibility issue.
Why it surfaces somewhere else entirely
Healthcare has a long history of attributing costs to the visible problem rather than the upstream cause. It is how EHR adoption went for a decade: the workflow pain was real, the source of the pain was often the integration gaps nobody planned for, and the conversation stayed focused on user adoption because that was the thing on the screen.
The same pattern runs through workforce operations. When a premium labor line item shows up in a variance report, the conversation that follows is about staffing budget, agency rates, and fill ratios. It is almost never about the credentialing visibility window that set the sequence in motion, because that event is four steps back and three systems removed from the report anyone is reading.
NCQA's 2025 credentialing standard updates tightened verification windows and added continuous monitoring requirements for accredited organizations, effective for files processed on or after July 1, 2025. The intent is right. Faster, tighter, more current credentialing. The work to get there is real, and most organizations I talk to are in the middle of it. What those updates don't address on their own is the handoff: what happens between when the credentialing work is done and when that status is legible to the scheduling workflow that needs it.
The broader industry baseline still puts hospital credentialing and privileging at 90 to 180 days from initial application to a fully privileged status visible to scheduling. The NCQA updates compress the front end of that. They don't close the operational gap at the back.
Timing is the actual variable
Privileging delays are often measured in days. Staffing decisions happen in hours. That mismatch matters more than the volume of credentialing work itself.
If a clinician becomes available on Friday morning and the shift was escalated externally on Thursday afternoon, the decision doesn't reverse. The external coverage is already secured. The cost is already committed. One event doesn't move the needle much. Repeated over weeks and across sites, it starts to reshape behavior in ways that are harder to undo. Teams begin to assume certain roles or locations just require external coverage, because in their experience, they always have. The assumption isn't wrong based on what they've seen. It's just based on incomplete information, systematically.
What the CAQH Index has been tracking for over a decade is the administrative cost embedded in manual credentialing and enrollment work, which runs into the tens of billions annually across the U.S. healthcare system. That framing is important. The piece that gets less focus is the downstream operational cost that shows up in coverage decisions made without the full picture. Those costs don't land in administrative budgets. They land in premium labor lines, in hiring plans that don't pay back on schedule, and in workforce programs that look less effective than they actually are.
What actually changes when privileging becomes visible at the decision moment
The change isn't about credentialing faster, though speed helps. It's about credentialing being legible to the workflow that uses it, at the moment the workflow needs it.
When a credential update is visible in scheduling the day it is finalized, the coverage decision that comes up that afternoon includes that clinician as an option. New hires contribute sooner because their eligibility shows up in the scheduling view as soon as it is true, not a week after. Cross-site capacity becomes usable because the privilege status is current across the systems reading it.
External coverage stays part of the picture. It moves from a default to a deliberate choice, used where it adds real value rather than as the answer to a visibility gap. Premium labor spend tends to settle as a result, not because of headcount changes, but because the internal investment starts working the way it was supposed to.
That is the operational gap Kimedics was built around. We bring credentialing status, privilege state, availability, eligibility, and scheduling into one operational view so the parties making coverage decisions can see what is actually true at the moment the decision is on the table.
The takeaway
A lot of what gets categorized as a staffing problem is, at the operational level, a privileging visibility problem. The credential is done. The privilege is current. The scheduling workflow doesn't know it yet.
Closing that gap is quiet, slow, unglamorous work. It also tends to be where the most durable operational change happens. The workforce doesn't change. The timing does.
How Kimedics helps
Kimedics connects privileging, readiness, and scheduling into one shared view.
Teams can see when providers are becoming deployable and act on that information before decisions move forward without them.
This reduces the gap between approval and utilization, helping organizations make better use of the capacity they already have.
Q&A
Q: What is a privileging delay, and why does it matter to scheduling?
Privileging delay is the lag between when a clinician's credential or privilege is finalized in the credentialing system and when that status is actually visible in the workflows used to make coverage decisions. The credentialing work may be complete. The information has not yet reached the people making the scheduling call. In most organizations, that lag is measured in days. Coverage decisions are made in hours. The mismatch is where capacity gets lost.
Q: How does this show up in variance reports?
It usually doesn't, at least not directly. The event that traces back to a privileging delay shows up on the report as a premium labor line or an external coverage cost. The privileging event that set it in motion is three steps back and rarely in the same view. That's why it stays in the conversation about staffing budget rather than credentialing workflow.
Q: Isn't this a credentialing process problem, not a staffing problem?
Both, and the line between them is where most of the cost actually forms. The credentialing process work matters and the NCQA 2025 updates are moving it in the right direction. The operational disruption happens at the handoff, when credentialing information needs to become legible inside the scheduling workflow on the same timeline as the decisions depending on it. Improving the process upstream is necessary. Closing the handoff gap is a separate problem.
Q: Does this apply to staffing agencies as well as health systems?
Yes, and it's often sharper on the agency side. An agency coordinator managing placements across multiple client sites is working with privilege status information that may be current in one system and two days stale in another. The scheduler at the health system is working from whatever is visible in their system. When those two views don't match in real time, the handoff breaks down quietly.
Q: What does Kimedics actually do differently here?
Kimedics is the clinician workforce operations platform built by healthcare operators. The platform brings credentialing status, privilege state, availability, eligibility, and scheduling into one operational view, so the people making coverage decisions on both sides of the relationship are working from the same current picture. We don't replace credentialing. We carry the result of that work into the workflow that uses it, with the timing the decision needs.
Ready to reduce delays between approval and deployment?
Speak to the team
Learn more about Kimedics
Kimedics is the clinician workforce operations platform built by healthcare operators. It was designed by people who have lived on the operational side of this industry and understand what each party actually needs from the workflow. We help healthcare organizations gain visibility across internal and external staffing to reduce complexity and improve financial performance. For more information, book a demo or email kimedics@kimedics.com